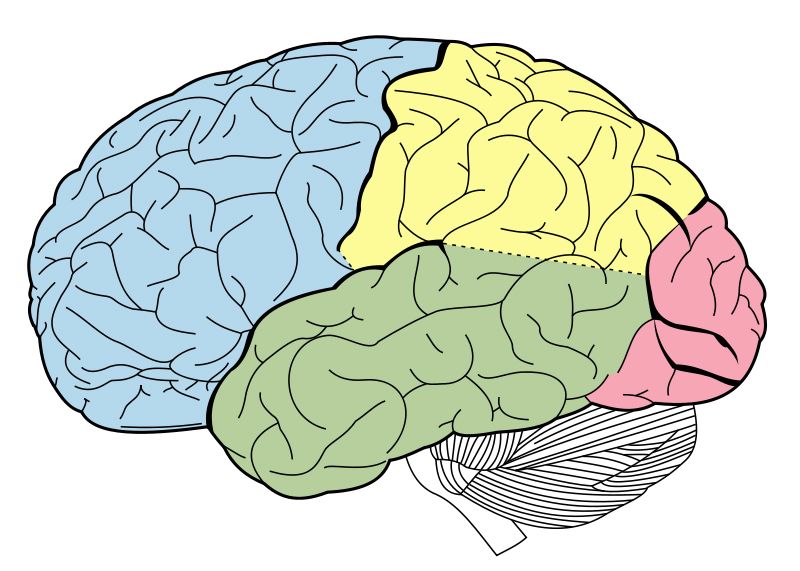
In the last two posts for Medical Monday I have outlined the basic anatomy of the brain and have given an overview of some of the differences between a typical brain and one with Down syndrome. Today's post is about some of the research that is going on that concerns Down syndrome and why that is significant.
 One of the major areas affected by Down syndrome is the hippocampus, which is largely tasked with spacial skills and memory creation/consolidation. As there are three copies of chromosome 21 with Down syndrome (Trisomy 21), one theory is that it is an over expression of specific genes which causes some of the major cognitive difficulties.
One of the major areas affected by Down syndrome is the hippocampus, which is largely tasked with spacial skills and memory creation/consolidation. As there are three copies of chromosome 21 with Down syndrome (Trisomy 21), one theory is that it is an over expression of specific genes which causes some of the major cognitive difficulties. If the specific genes themselves, cellular activity created by these genes or even a protein or compound secreted/lacking from the cells can be targeted, some of the cognitive problems with DS can be alleviated (or so the theory goes). Most of the study in this area however, could not be accomplished without a very special mouse.
The Down syndrome Mouse Model
 |
| Photo courtesy of Stanford School of Medicine, Down Syndrome Research Center |
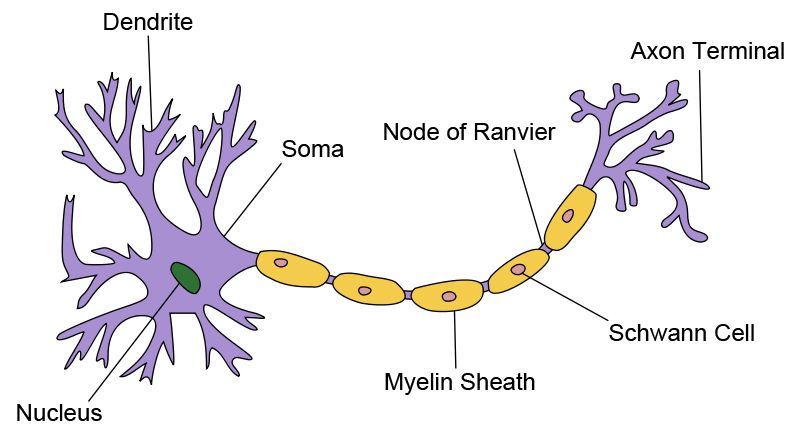
Having a model to help understand things like cognition has proved to be infinitely helpful and has opened many new avenues of research into Down syndrome, cognition and aging. Included are: the excitation/inhibition of certain neural pathways, restoring neuronal pathways, neurotransmitter restoration, sleep abnormalities and the discovery/reassignment of drugs for treatment (for more information regarding specific American projects, see this listing, courtesy of the Down Syndrome Research and Treatment Foundation. For a Canadian listing, see the Down Syndrome Research Foundation).
Down Syndrome and Alzheimer Disease
Alzheimer Disease is the most common form of dementia and has a very early onset in the Down syndrome community. As a result, these two areas of research are frequently joined; finding out what mechanism causes Alzheimers could lead for a treatment for both the general population and those with DS.
Dr. William Mobley is a Distinguished Professor and Chair of the Department of Neurosciences at UCSD and the Executive Director of UCSD's Down Syndrome Center for Research and Treatment. In this video, you can see Dr. Mobley discuss not only the mouse model that he uses in his research but also the link between Alzheimers and Down Syndrome and what these findings will mean for people with DS (from 6:26 on).
(Video courtesy of UCSD-TV)
More Information and Donating to DS Research
Sadly, Down syndrome research is chronically underfunded.
If you are interested in learning more or possibly participating or helping out DS research there are a variety of foundations through which you can do so (including the Down Syndrome Research Foundation in Canada and The Down Syndrome Research and Treatment Foundation in the US).
One of the more enjoyable organizations has been the DSRTF's +15 Campaign. Not only do they offer up a voice for research, but they also raise funds for ongoing studies. With a goal of increasing the cognitive abilities of those with Down syndrome 15 percent (which could mean the difference between a person living on their own or not, for example), they have a variety of ways in which to stay abreast of current research trends. Interested parties can donate $15 (or more) directly to DS research or if you wish to "Adopt-a-Mouse", host an event or simply raise awareness, those options are available as well.
Understanding Down syndrome and increasing the cognitive abilities of those with it are very close to being a reality. With ongoing research and new discoveries being made all the time, successful treatments could shortly be within our grasp.
+15 <http://www.plus15.org/>
Down Syndrome Research Foundation <http://www.dsrf.org/>
Down Syndrome Research and Treatment Foundation <http://www.dsrtf.org/page.aspx?pid=291>
Jarrold, Christopher, Lynn Nadel, and Stefano Vicari. "Memory and Neuropsychology in Down Syndrome." Down Syndrome Education International (2007): n. pag. Web. <http://www.down-syndrome.org/>.
Heyn, Sietske. "The Down Syndrome Mouse - A Historical Perspective & What the Future May Hold." Stanford School of Medicine Down Syndrome Research Center. Stanford School of Medicine, n.d. Web. <http://med.stanford.edu/>.
Stanford School of Medicine, Down Syndrome Research Center <http://med.stanford.edu/>
UC San Diego School of Medicine, Department of Neurosciences <http://neurosciences.ucsd.edu/Pages/default.aspx>