As current data suggests that DS occurs in 1 out of every 700 or so births, you would think someone would have noticed it before 1858 (perhaps in every culture since the dawn of time). That would be correct. As Down syndrome has been stigmatized and de-stigmatized at several points in human history, the physical evidence is few and far between. However, it is still there.
From Prehistory
There are several instances of material evidence from prehistory that experts believe depict Down syndrome. Clay tablets from Babylon dating back to 4000 BC record congenital 'malformations'. Included are 62 human 'malformations' (and associated prophetic relations). There is evidence from the Paleolithic era (18,000 years ago) which may depict Down syndrome or a related condition.
Taurodontism has been found in two teeth of this era, which is often associated with chromosomal disorders such as trisomy 21. (Savona-Ventura, ?). A skull from a monastery at
Breedon-on-the-hill in North West Leicestershire in England dates to approximately 700-900 AD and is alleged to have numerous features typically seen in individuals with Down syndrome. Among those listed are an overall reduced size,
microcephaly,
a smaller skull cap, small
maxilla, smaller skull length,
thin cranial vault bones, smaller face and
cheek bones,
brachycephaly, thick
mandible,
mandibular prognathism and irregular
tooth development. (Starbuck, 2011).
 |
| Tolteca terracotta figurine |
This terracotta figurine from Mexico dates to the Tolteca culture (approximately 500 AD) and depicts facial features that suggest Down syndrome: small, up-slanting eyes, a small face, noticeable tongue, a weak nasal bridge and an open mouth.
 |
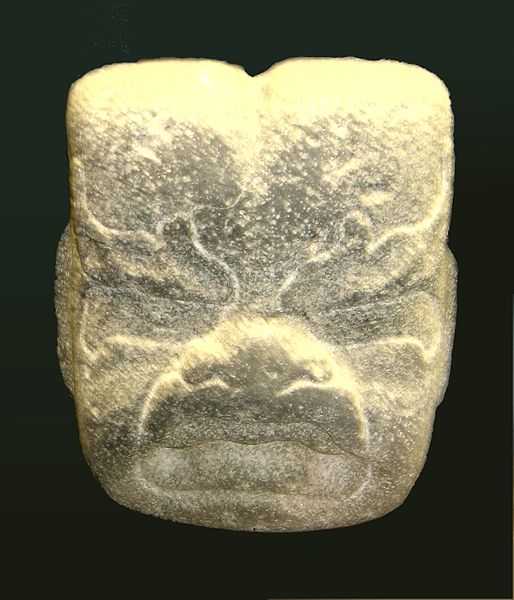
| Olmec Were-Jaguar |
 |
| Olmec mother holding jaguar child |
One of the more disputed theories lies with the Olmec culture (also of Mexico) which existed from roughly 1500 BC to 300 AD. The surviving art of this culture often depict jaguars mating with older women of the tribe to produce 'jaguar-babies' or '
were-jaguars'. It has been put forth by numerous sources that these 'jaguar babies' probably had Down syndrome based on the fact that they were a) born to older women, b) were depicted with sharp teeth (possibly
ectodermal dysplasia), c) had small, slanted eyes, d) had flattened noses, e) were often rounder or more overweight than other representations of children (
hypotonia and
hypothyroidism) f) were often depicted in unusually flexible positions (suggesting
hypermobility), g) when depicted as infants, were depicted limp (hypotonia again) and h) had cleft heads (enlarged
metopic suture). Again, the physical evidence is moderate at best making this a widely disputed argument in the anthropological world.
The Tumaco-La Tolita culture of Columbia and Ecuador (600 BC to 350 AD) is known for depicting a variety of diseases and ailments in their work. One figurine in particular is suggestive of Down syndrome (Bernal, Brecino, 2006 and Starbuck, 2011) as it depicts a short, obese person with small, up slanted eyes, an open mouth, a small nose with depressed bridge, a small face relative to the rest of the head, a protruding jaw and thickened fingers.
Historical Evidence Potentially Depicting Down syndrome
One of the oldest is a painting from roughly 1505 referred to as "
Ecce-homo-scene". It has been put forth that the child depicted in this painting has the characteristics of Down syndrome. The eyes are small and slightly up slanted, the neck is broad, the ears small and low set, the face small compared to the rest of the head, there is a weak nasal bridge, the mouth is open and there is an overall stocky appearance. It could be inferred from this painting that the child is a type of street performer; in fact there is a monkey on a leash which is grooming the child's hair. Sadly, this last aspect would fit with the times. (Starbuck, 2001)
The next are a series of religious paintings that have been attributed to Andrea Mantegna (1431-1536). The first,
Virgin and Child with Saints Jerome and Louis of Toulouse (approx 1455 AD) depicts a child with up slanted small, widely spaced eyes, an open mouth with a protruding tongue, short digits with an in-curving 5th finger and a weak nasal bridge with a "button" nose. Also notable is the hypotonic or relaxed facial expression.
Around 1460, Mantegna created
Madonna and Child which has also been suggested to exhibit characteristics of Down syndrome: epicanthal folds, small narrow eyes, an open mouth, hypotonic expression, flattened nasal bridge and button nose.
Also from (approx.) 1460 AD, is a painting entitled
Virgin and Child which experts believe to also exhibit characteristics of Down syndrome. Among those listed are: epicanthic folds, oblique eyes, open mouth, protruding tongue, in-curving 5th finger, widely spaced first and second toe, a smaller head, a short, broad neck and hypotonic facial expression.
It has been suggested that the reason for several of his paintings having children with Down syndrome features (while others notably do not) is due to the claim that one of Mantegna's 14 children had Down syndrome and one of his patrons, the Gonzanga family, also had a child with Down syndrome (which reportedly died at four years of age). (Starbuck, 2011)
One of the most famous examples is found in the Flemish painting
The Adoration of the Christ Child, created around 1515 by a follower of Jan Joest of Kalkar. There are two individuals in this painting that have strikingly different facial features than the others and it has been argued that they depict people with Down syndrome.
The first figure is an angel to the right of the Madonna. Unlike the Madonna, the angel figure displays a flatter than normal face, up-slanting narrow eyes, epicanthic folds, flattened nasal bridge, upturned button nose, a downturned mouth and shorter than normal digits.
The second figure is a shepherd boy located in the background. It has very similar features to the previous angel (ie: flatter face, up-slanting narrow eyes, epicanthic folds, a flat nasal bridge, a button nose and a downward turned mouth). This figure however, also has widely spaced eyes and a hypotonic expression on the face. It is to be noted that there is a
second "daytime" version of this painting where these characters are more typical looking. (Starbuck, 2001)
It is well known that those with disabilities, both learning and otherwise have been scorned, ridiculed and even regarded as evil throughout the ages. Even Aristotle stated in his Politics: "
...as to the exposure and rearing of children, let there be a law that no deformed child shall live." This has persisted right up to modern day and beyond John Langdon Down. With this artistic evidence, it makes one wonder if not everyone felt this way. Aside from the were-jaguars, it is interesting that there are two separate versions of the Adoration of the Christ child and that the infant Jesus was depicted in such a manner. I would like to think that this would suggest that small pockets of free thinkers, small groups of people who were touched by Down syndrome saw beauty, not an abomination. I would like to think that there have been people throughout history that did not fear and despise those that were different, but rather saw them as something special. So much so that they would depict their 'Savior' with those same characteristics.
------------
Bernal, J. E., and I. Briceno, 2006
Genetic and other diseases in the pottery of Tumaco-La Tolita culture in Colombia-Ecuador, Clinical Genetics, 2006
Savona-Ventura, Charles ( )
Historical Perspective Congenital Malformations: a historical perspective in a Mediterranean community
Starbuck, JM
, On the Antiquity of Trisomy 21: Moving Towards a Quantitative Diagnosis of Down Syndrome in Historic Material Culture, Journal of Contemporary Anthropology, October 2011
------------